The OrthoTiN TMJ system is designed with focus on matching patient unique anatomy.
The implants geometry is based on the 3D skull model that is generated from the CT Scan of the specific patient.
OrthoTiN Prosthesis are intended to provide a custom bone fitting surface replacements for the joint maintaining maximum bone stock.
One of the advantages of a custom system is the familiarity of the patient’s anatomy that the design team develops throughout the generation of the anatomical model as well as the prosthesis design. Using OrthoTiN’s CT scan protocol results in scan data that best approximates patient anatomy and leads to a more accurate device. With an accurate representation of the patient’s maxilla and mandible anatomy, surgical planning becomes more accessible and reliable. Osteotomy planning, occlusion adjustment, and any patient specific considerations can be addressed. Anatomical biomodels are supplied for verification of the design and used intraoperatively during the implantation of the prostheses in the virtually planned position.
Custom surgical guides aid drilling pilot holes, the condylectomy and the planned occlusion.
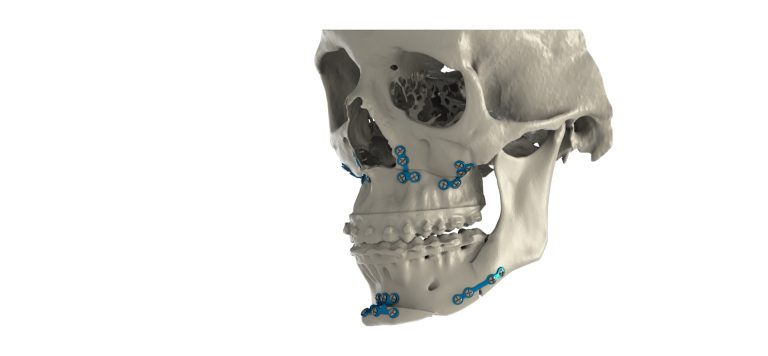
Our TMJ system can be used for combination cases with orthognathic to reduce the need for separate procedures and provide holistic planning options.

The prostheses are divided into a fossa and ramus component.
The fossa is comprised of a solid Titanium Alloy fossa component and a Polyethylene bearing that interlock together to serve as the anatomical glenoid fossa and articulate with the ramus prosthetic condylar head.
A patient-specific fossa component makes complete contact with the anatomical surface, creates stability, and reduces micromotion. Stress within the component is reduced by efficiently transferring joint loads to the bone. In cases where a patient has anatomical deficits, the custom component is made for their unique circumstances.
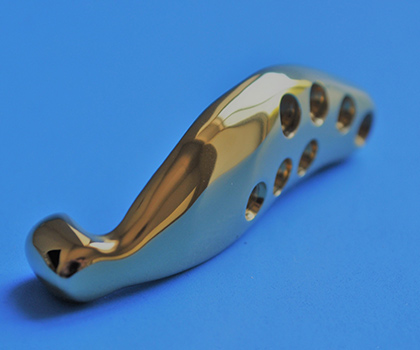
The ramus is also made using Titanium Alloy and it coated with a ceramic Titanium Nitride coating to greatly improve wear resistance on the articulating surface. This component is made specifically to match the patient’s anatomical ramus.
A standard flat ramus component may not be suitable for patients with irregularly shaped mandibular anatomy. Custom components allow for control over the shape of the condylar component, the flexibility of positioning of the screws, and the adaptation of the internal surface. Designs can be altered to increase fixation, adjust screw positioning, accommodate best bone stock, and to avoid interference with soft tissue. If the occlusion can be improved by adjusting the position of the mandible, the design of the ramus component can be altered accordingly.

One of the many benefits of patient specific joint replacement is for challenging cases extended prostheses can be manufactured.

The standard design for the condyle in the OrthoTiN TMJ prosthesis is a modified barrel shape which allows for line contact between the condylar head and the UHMWPE bearing surface. This shape allows for greater contact area and disbursement of load as compared to the traditional ball design, which uses point contact. The barrel is bevelled on either side to allow for a greater range of motion and to adapt a superior fit to the condylar surface. The increased contact area decreases the wear of the polyethylene bearing. Mathematical analysis shows an approximate ten-fold decrease in load disbursement, which offers a significant biomechanical advantage over conventional ball on flat surface.
The advantages of titanium alloy over the traditional Co-Cr alloy used are numerous. The increased flexibility of titanium alloy allows for more of the load to be carried by the bone, reducing stress protection of the bone. Titanium alloy is also more biocompatible than Co-Cr alloy, whose major components can be carcinogenic. Titanium alloy is stronger than Co-Cr alloy in fatigue and yield resistance. The main disadvantage of titanium alloy is its inferior abrasion resistance, a problem minimized with the use of the extremely hard TiN coating. With the use of C-TiN-C, there is no need for a Co-Cr condylar head, which eliminates the metal-metal interface. Orthopedic specimens with modular heads have shown a disturbing degree of corrosion at the connection interface, as a result of micromotion in the interface (fretting corrosion). This issue is functionally eliminated by the one-piece condylar design, also have the benefit of reducing prosthesis cost and enhancing overall strength.

Lyka Smith will supply our TMJ screw instrument set with every case.
There is little consensus on how to evaluate and manage patients reporting a possible material sensitivity to joint replacement devices containing metal. The specific material composition of the OrthoTiN implant components can be found elsewhere on our webpage. There are 2 tests that can be used to evaluate patients for hypersensitivity: skin patch testing (SPT) and the lymphocyte transformation test (LTT). However, there is no agreement on the best timing and under what clinical circumstances a patient should undergo a hypersensitivity workup. The skin patch test has not been shown to be a reliable indicator of metal implant hypersensitivity. Before a primary total joint replacement, testing can be helpful when a patient reports a history of intolerance to jewelry or of an allergic reaction to a prior metal implant. However, to date, routine testing is not supported by the literature. Currently, the diagnosis of hypersensitivity to metal implants appears to be one of exclusion and there are no available clear-cut management algorithms. Based on a review of the available orthopedic literature, a practical workup and management of potential material hypersensitivity algorithm for pre and post op patients was developed. (see, Mercuri LG, Caicedo MS. Material Hypersensitivity and TMJ Replacement. J Oral Maxillofac Surg 77:1371-1376, 2019.) OrthoTiN is only able to provide a limited quantity of all-titanium mandibular implants via the FDA’s compassionate use program for documented highly reactive material sensitive patients. Please consult with us regarding ordering All-Ti implants for details on this process.
TMJ replacement should always be performed first in combined maxillary and OrthoTiN cases. If the maxilla is performed first, and not positioned in the exact pre-surgically designed position, the custom OrthoTiN components may not interface properly with the host bone nor articulate appropriately.
OrthoTiN TMJ Implants are made from Titanium Alloy. Titanium has many desirable characteristics; it is considered to be more biocompatible, has closer mechanical properties to that of bone than cobalt-chromium alloys used in other TMJ systems. Titanium alloy is widely considered the material of choice for orthopedic implants. Unfortunately, titanium is much less abrasion resistant in comparison to Co-Cr. To improve the hardness, and enhance biocompatibility of the titanium implants, the OrthoTin mandibular ramus component is coated with a titanium nitride coating. This coating results in an increased lubricity, improved durability, abrasion resistance, as well as improved hardness. A reduction in component wear leads to a reduction in metal ion release – reduced Nickel exposure. Studies demonstrate that Titanium Nitride coating reduces wear on UHMWPe by two thirds when compared to a cobalt-chromium alloy. In addition, the wear rates associated with a TiN Coat / UHMWPe interface are very minimal. The low wear rates, biocompatibility, and desirable mechanical properties of TiN coated titanium alloy devices show promise for the potential longevity of the OrthoTiN TMJ System.